CADASIL is one of the few identified causes of hereditary disease in the small cerebral arteries. It is transmitted in an autosomal dominant manner. Some cases appear to be sporadic, with de novo mutations in a patient although neither of the parents are carriers of the mutation.
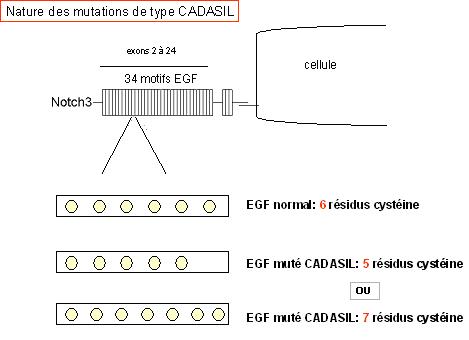
To be certain of diagnosis, molecular screening is required. The gene implicated in the disease is the Notch3 gene located on the short arm of chromosome 19. It consists of 33 exons including 23 exons (from 2 to 24) which code for EFG-like patterns containing six cysteine residues.
To date, all the mutations responsible for the disease have been located within these exons (2 to 24). They are very sterotyped and all of them lead to either the gain or loss of cysteine in one of the EGF-like patterns. The presence of this type of mutation confirms the diagnosis beyond all doubt.
In 50% to 70% of cases in the French population, the mutation is located in exons 3 or 4 of the Notch3 gene and, in more than 98% of cases, the mutation is located in one of the 15 following exons: 2, 3, 4, 5, 6, 7, 8, 11, 12, 18, 19, 20, 21, 22, or 23.
meet demand from clinicians who suspect CADASIL in patients, our laboratory has introduced routine sequencing of the 23 exons coding for EGF-like patterns in the Notch3 gene.
- The screening of the 23 exons coding for EGF areas on Notch3 is estimated to be almost 100% sensitive.
For asymptomatic adults at risk of the disease who ask for molecular testing, it is essential for them to attend a multidisciplinary consultation before any final decision is made. Screening is not currently prescribed for asymptomatic minors.
N.B.: immunohistochemical analysis of skin biopsies is no longer carried out.








